


 Sign Out
Sign Out



Sympathomimetic Agents: Concomitant administration of other sympathomimetic agents (alone or as part of combination therapy) may potentiate the undesirable effects of TRELEGY ELLIPTA (see Precautions).
Treatments Leading to Hypokalaemia: Beta-agonists have been associated with reductions in serum potassium levels. Concomitant treatment with xanthine derivatives, oral corticosteroids (e.g., prednisone), or non-potassium sparing diuretics may potentiate any hypokalemic effect of adrenergic agonists (see Endocrine and Metabolism, and Hypokalemia and Hyperglycemia under Precautions).
Beta-Adrenergic Blockers: Beta-adrenergic blockers may weaken or antagonize the effect of beta2-adrenergic agonists, such as vilanterol. Therefore, TRELEGY ELLIPTA should not be given together with beta-adrenergic blockers (including eye-drops) unless there are compelling reasons for their use. In this setting, cardioselective beta-blockers could be considered, although they should be administered with caution.
Metabolic and transporter based drug interactions: Fluticasone furoate and vilanterol are both substrates of CYP3A4.
Co-treatment of fluticasone furoate with CYP3A4 inhibitors is expected to increase the risk of systemic side effects (see Table 9). Co-administration should be avoided unless the benefit outweighs the increased risk of systemic corticosteroid side effects, in which case patients should be monitored for systemic corticosteroid side effects.
Co-administration of repeat dose ketoconazole (a strong CYP3A4 inhibitor and P-gp inhibitor) with fluticasone furoate/vilanterol 200/25 mcg resulted in increased mean fluticasone furoate AUC(0-24) and Cmax by 36% and 33%, respectively, and increased mean vilanterol AUC(0-t') and Cmax by 65% and 22%, respectively. The increase in fluticasone furoate exposure was associated with a 27% reduction in weighted mean serum cortisol (0 to 24 hours). The increase in vilanterol exposure was not associated with an increase in beta-agonist-related systemic effects on heart rate or blood potassium but was associated with a slight increase in QTcF interval. Administration of inhaled vilanterol 25 mcg alone with ketoconazole 400 mg resulted in a 1.9-fold increase in vilanterol systemic exposure as measured by AUC(0-t), but there was no change in Cmax. The increase in AUC was not associated with effects on heart rate, blood potassium, and QTcF. Therefore, caution is required with the co-administration of TRELEGY ELLIPTA and ketoconazole or other potent CYP3A4 inhibitors.
Umeclidinium is a substrate of CYP2D6; however, umeclidinium pharmacokinetics were not significantly affected in a population of CYP2D6 poor metabolizers (Pharmacology: Pharmacokinetics under Actions).
Fluticasone furoate, umeclidinium and vilanterol are substrates of P-glycoprotein (P-gp). The effect of the moderate P-gp transporter inhibitor verapamil (240 mg once daily) on the steady-state pharmacokinetics of umeclidinium and vilanterol administered together and umeclidinium administered alone was assessed in healthy volunteers. An approximately 1.4-fold increase in umeclidinium AUC was observed with no effect on vilanterol AUC. No effect of verapamil was observed on umeclidinium or vilanterol Cmax. A decrease in blood potassium, an increase in QTc interval and an increased number of supraventricular tachycardia events occurred with co-administration with verapamil. No P-gp inhibitor drug interaction studies have been conducted with fluticasone furoate alone or in combination with vilanterol.
Drug-Drug Interactions: The drugs listed in Table 9 are based on either drug interaction case reports or studies, or potential interactions due to the expected magnitude and seriousness of the interaction (i.e., those identified as contraindicated). (See Table 9.)
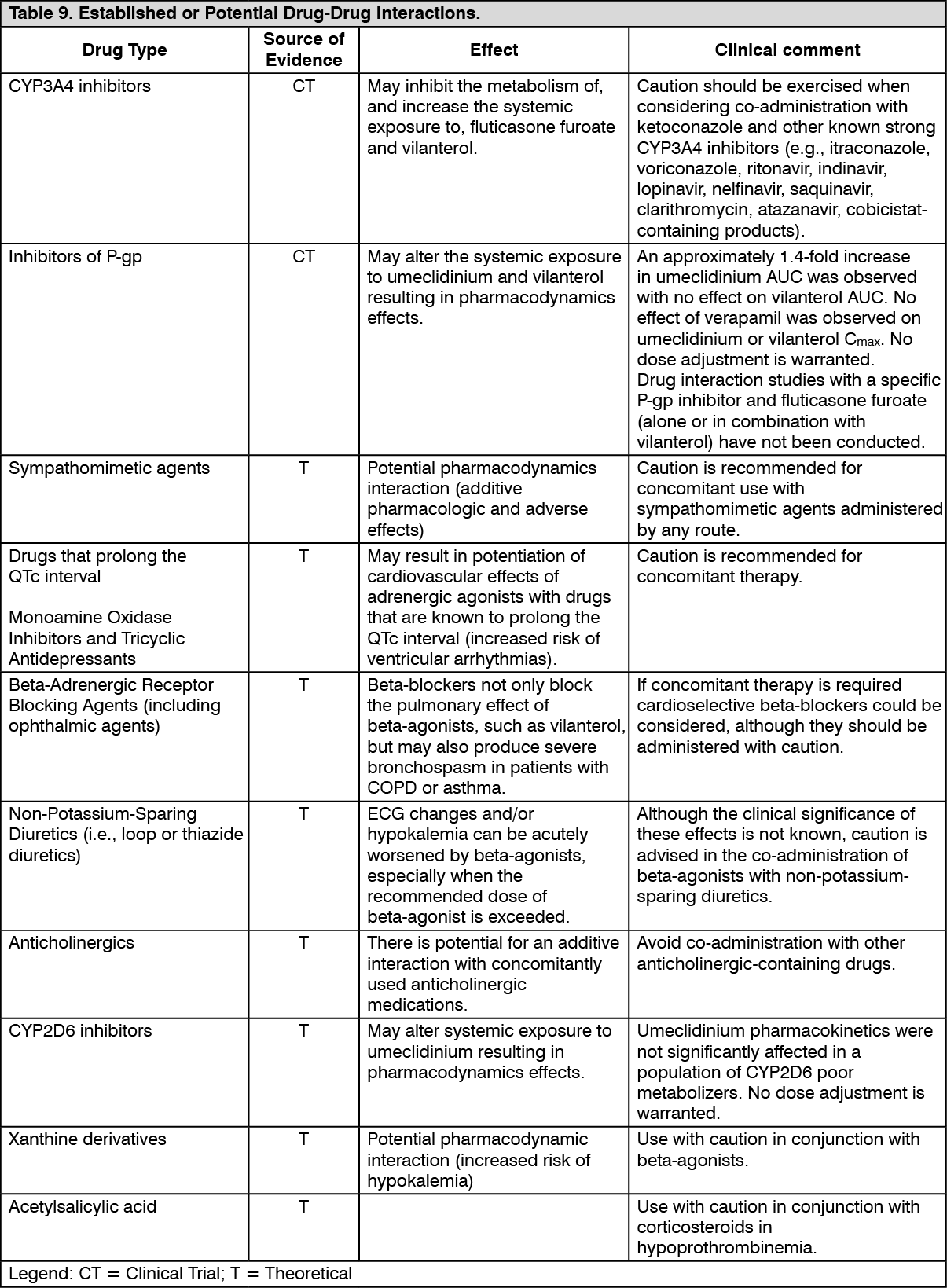 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageDrug-Food Interactions: Interactions with food have not been evaluated. No clinically relevant effect of food would be expected and therefore a food interaction study was not performed.
Drug-Herb Interactions: Interactions with herbal products have not been evaluated.
Drug-Laboratory Test Interactions: Interactions with herbal products have not been evaluated.